Novel algorithms for the pragmatic use of ultrasound in the management of patients with rheumatoid arthritis: from diagnosis to remission pdf



Targeting ultrasound remission in early rheumatoid arthritis: the results of the TaSER study, a randomised clinical trial pdf
Percentage attainment of response criteria after 18 months follow-up:
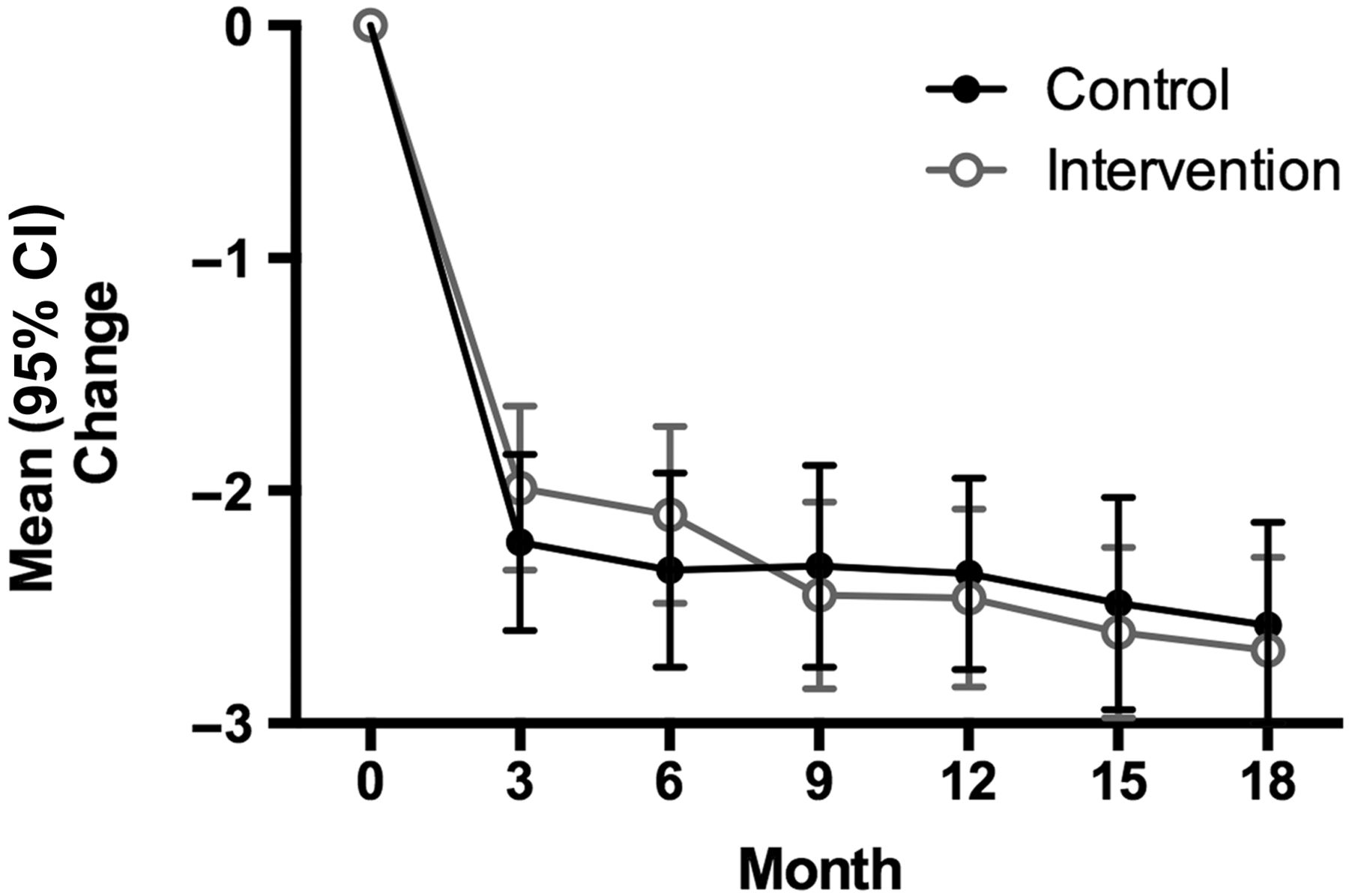
Median Health Assessment Questionnaire (HAQ). (†p=0.31, ††p=0.06):
Ultrasound guidance of early RA therapy doesn’t improve outcomes
Ultrasound in management of rheumatoid arthritis: ARCTIC randomised controlled strategy trial pdf


ARCTIC Study Shows No Benefit to Ultrasound Remission in RA
Systemic ultrasound in the management of early rheumatoid arthritis is not justified
Is it time to revisit the role of ultrasound in rheumatoid arthritis management? pdf

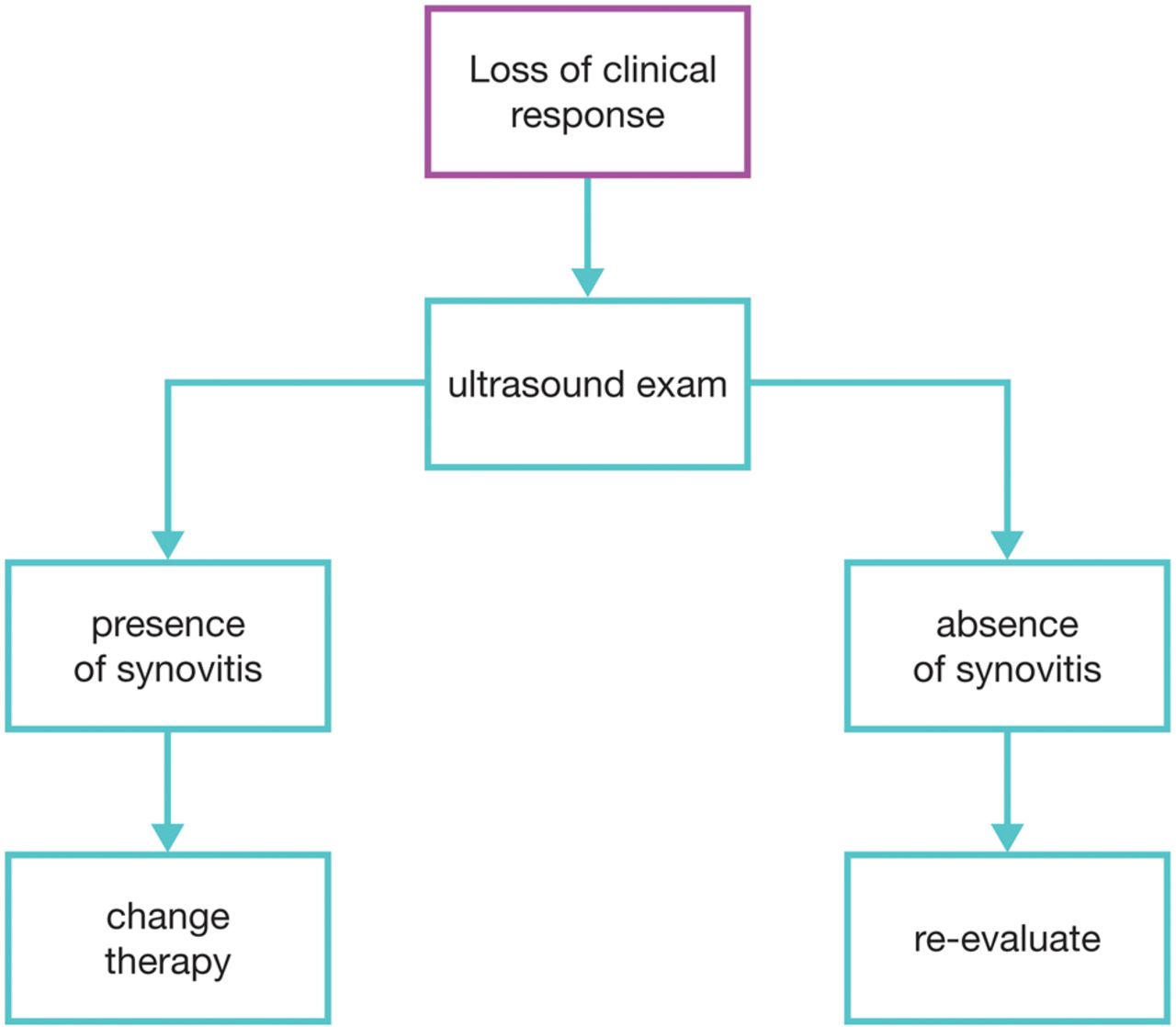
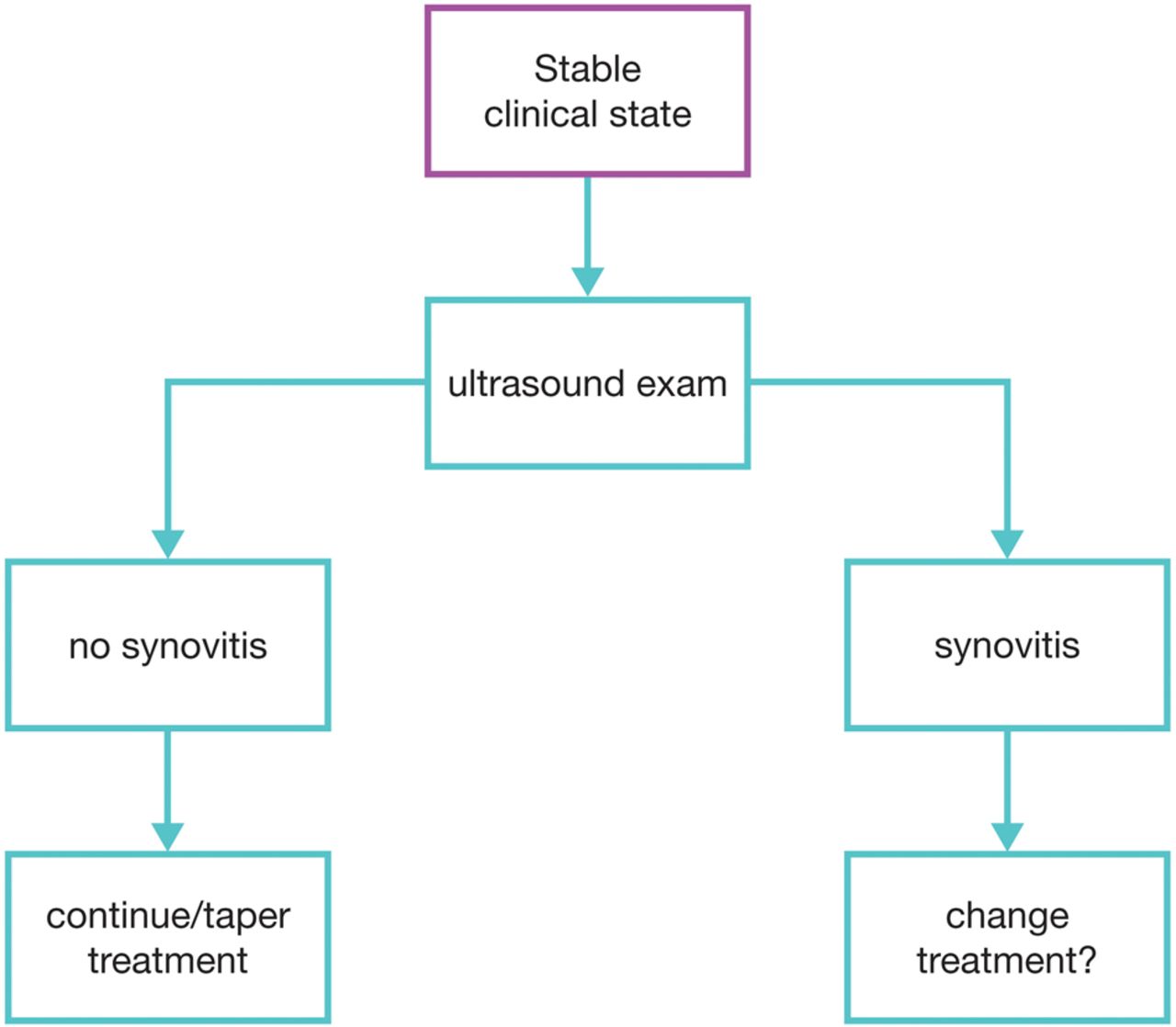
Ultrasound, especially power Doppler (PDUS), has demonstrated its usefulness in the entire range of RA management, from early diagnosis, to monitoring, to tapering, and to flare. The only controversial link in this chain is in guiding treatment intensity to achieve disease remission. That’s owing to 2 recently published landmark trials: TaSER and ARCTIC.
On cursory reading (especially if all you read are the abstracts’ conclusions), then you’ll conclude that using ultrasound to guide therapy results in higher costs (more man-hours spent scanning the joints; higher usage of costly biologics) without a commensurate or better remission rate compared to current standard-of-care (which uses clinical outcome measures to guide therapy).
To be fair, current standard-of-care is really very good. Because of tight disease activity control, we as rheumatologists no longer see RA patients with joint deformities commonly shown in textbooks. Therefore, for ultrasound to better that is a tall order to begin with.
However, if you read the detailed results in the 2 studies, you’ll find that ultrasound-guided (USG) treat-to-target (T2T) yielded numerically superior scores in remission rates as well as clinical outcome measures like disease activity scores, albeit the differences were not statistically significant (with the exception of DAS44 remission at 18 months in TaSER). Interestingly, when you look at patient reported outcomes (PRO) like function and quality of life, USG-T2T (HAQ in TaSER) showed a trend towards superiority by 18 months, which was almost statistically significant. And in ARCTIC, USG-T2T appeared to significantly retard radiographic progression (joint damage) after 2 years in the roughly 15% of patients with more severe disease (called the “rapid progressors”).
The interpretation of these results continues to be hotly debated among rheumatologists. I think the following points complicate the interpretation:
1) As mentioned earlier, the comparator is active tight control, which is very effective in achieving clinical remission as is;
2) USG-T2T is driven mainly by PDUS, and the current semi-quantitative grading system (0-3) is not clear on what grade constitutes clinically significant inflammation deserving of treatment escalation (grade 1 or 2?), and inter-rater reliability remains weak between grades 2 & 3;
3) To define a primary remission endpoint in terms of the comparator’s targeting strategy is problematic, it’s like using a yardstick to measure the yardstick. Are the current clinical remission criteria (EULAR Boolean, DAS28/44, SDAI, etc) or even the radiographic outcome (modified Sharp score) the ultimate target? I posit that PROs are more clinically meaningful and therefore ultimately more relevant and important. I made reference to this in my earlier “MRI in RA” post, and shall be elaborating on it in a later post on “PRO in RA”.
Given my perspective, my take-home on TaSER and ARCTIC are:
1) Imaging (PDUS & MRI) allows for targeting a deeper remission than clinical outcome measures;
2) A deeper remission which is sustained is needed to improve PRO, which is a more important target than clinical remission;
3) USG-T2T is unnecessary for every RA patient at every review, especially if the patient reports to be doing well enough (not keen for therapeutic adjustments), even if the physician global assessment is in discordance. Instead, it should be reserved for monitoring the small proportion of rapid progressors.