A Few Good Meds #4: RITUXIMAB
In present day rheumatological practice, Rituximab is both Lifestyle Med and Drug of Last Resort.
It is Lifestyle Med especially for the approved indications of RA and ANCA-Vasculitis (specifically Wegener’s Granulomatosis & Microscopic Polyangiitis), in that, with just 2 infusions a year, it can:
1) replace more toxic drugs like Cyclophosphamide and prolonged high dose steroids for effective induction of remission;
2) replace daily medications (hassle + constant immunosuppression risks) like Azathioprine and Methotrexate in maintaining remission.
What’s not to like? Like Tofacitinib, the cost $$$$$
But if you have the dough or a comprehensive medical insurance, it’s pretty lifestyle.
It certainly is Drug of Last Resort. Just look at the long list of off label usage; and the list keeps growing.
Even in diseases not known to be B-cell driven, like Ankylosing Spondylitis, we find it being tried and trialed, and surprisingly with subgroup efficacy (in anti-TNF naive patients). Perhaps it has a mode of action beyond mere B-cell depletion; either that or B-cells play a pathogenic role in such diseases after all.
What is most jaw-dropping is to behold the depths of desperation some descend to to use RTX in Chronic Fatigue Syndrome!
A Few Good Meds #4: RITUXIMAB in Chronic Fatigue Syndrome
It is often quipped that no rheumatic drug is totally useless until it has been tried in Scleroderma. The converse may also be said that no rheumatic disease is totally refractory until it has tried Rituximab. But, CFS, seriously?
A Few Good Meds #4: RITUXIMAB in ANCA-associated vasculitis
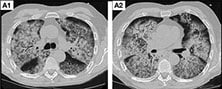
The RAVE trial and others have paved the way for Rituximab to revolutionise the management of ANCA-associated vasculitides, serving as both induction as well as maintenance of remission.
A Few Good Meds #4: RITUXIMAB in Systemic Lupus Erythematosus
Perhaps the most off-label use of Rituximab is in SLE, especially for Lupus Nephritis. As in other refractory systemic connective tissue diseases like Scleroderma and Dermatomyositis, RTX is the last stop before contemplating ablative chemotherapy with haemopoietic stem cell transplant.
A Few Good Meds #4: RITUXIMAB in Rheumatoid Arthritis
Amongst rheumatic diseases, RTX is most commonly used in RA. Although not (yet) indicated for use as a first line biologic, emerging evidence is changing expert opinion, especially for ACPA-positive patients.
Re-treatment timing is still an art. This study, however, suggests that monitoring T-cell (rather than B-cell) repletion may help in this decision-making.
This observation raises some interesting questions. How does a targeted B-cell depletion therapy affect T-cells? Is it a direct pleiotropic effect unique to RTX, or common to other CD20-directed monoclonals as well? Or is it consequential to reduced B-cell antigen presentation to T-cells?
Whatever the case, T-cell numbers (and activity) appear more correlated with RA disease activity and impending flare.
Perhaps the same may apply to monitoring and preempting disease flare in ANCA-vasculitis?